About myeloma
Myeloma is a blood cancer that starts in the plasma cells of the bone marrow. Plasma cells normally produce proteins called immunoglobulins, which help fight infection. In myeloma, abnormal plasma cells accumulate in the bone marrow, leaving little room for the production of healthy blood cells. As a result, people with myeloma are often tired due to a low red blood cell count and may experience recurrent infections caused by faulty plasma cells.
Myeloma plasma cells make an abnormal immunoglobulin called paraprotein, M-Protein, M-spike or myeloma protein. These have no useful function. Paraproteins are found in the blood and/or the urine of most patients. They can build up in the kidneys and other organs, causing damage. Non-secretory myeloma is the exception. It doesn’t produce a paraprotein and is only found and monitored by scans and bone marrow biopsies.
Myeloma cells also produce a chemical that stimulates cells called osteoclasts. Osteoclasts break down bone tissue. Consequently, bone tissue breaks down faster than it can be rebuilt.
When left unmanaged, there is an increased risk of:
- bone fractures due to increased osteoclast activity
- bone pain due to weakened bones, especially the spine which can put pressure on nerves
- developing small holes in the bones, called lytic lesions, which weaken the bones
- hypercalcaemia which occurs when bones break down and calcium is released into the bloodstream. This can cause symptoms of confusion, nausea, constipation and weakness.
Who gets myeloma?
- 2600 Australians are diagnosed each year.
- 84% of people diagnosed are over 60 years of age.
- 72 years is the average age at diagnosis.
Prognosis of myeloma
A prognosis is an estimate your haematologist will make of the likely course and outcome of your disease. Myeloma is a treatable blood cancer, currently there is no cure. Your treatment team will discuss your prognosis and treatment options with you.
Understanding immunoglobulins
Immunoglobulins (Ig), also called antibodies, are made by our plasma cells. These are made in the bone marrow. In particular, immunoglobulins protect us from and help fight infection. In myeloma, lots of abnormal plasma cells are produced. These cells make abnormal immunoglobulins called paraproteins.
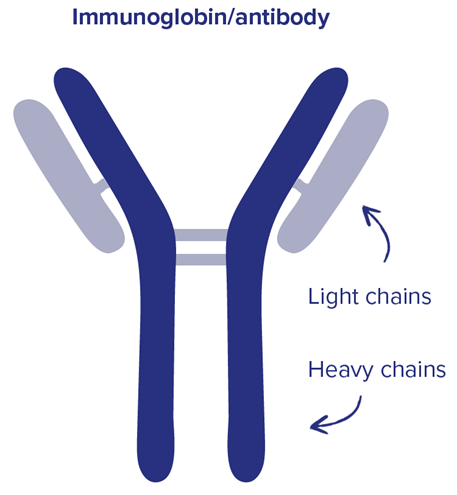
Each protein is made up of:
- heavy chains – two long protein chains
- light chains – two shorter protein chains.
There are different types of heavy and light chains:
- five types of heavy chains – G, A, D, E and M
- two types of light chains – kappa and lambda.
Your myeloma cells will produce a specific, single combination of one heavy chain type and one light chain type. For example, IgG kappa myeloma is the most common type of myeloma. It has two IgG heavy chains bound to two kappa light chains.
Some types of myeloma, like light chain or Bence Jones myeloma, only produce the light chain part of the paraprotein. These are called free light chains.
Causes of myeloma
There is no specific cause for myeloma. It is more common in men than women and the risk of developing myeloma increases with age.
Some factors that can increase your risk of developing myeloma include:
- a history of monoclonal gammopathy of undetermined significance (MGUS)
- family history of myeloma
- some viruses and autoimmune diseases
- radiation exposure – previous radiation therapy or high-level environmental radiation exposure
- hazardous chemicals – exposure to high levels of environmental chemicals.
Stages of myeloma
To work out your stage, your haematologist will look at some blood test results:
- beta-2 microglobulin – protein on myeloma cells
- albumin – protein in the blood
- lactate dehydrogenase (LDH) – indicates blood cell damage
- Fluorescent in-situ hybridisation (FISH) – cytogenetic test to look at chromosomes.
| R-ISS stage | Beta-2 microglobulin level (mg/L) | Albumin level (g/dL) | Lactate dehydrogenase (LDH) level | Chromosomes |
|---|---|---|---|---|
| Stage 1 Low risk | Less than 3.5 | Greater than or equal to 3.5 | Normal | No high risk chromosomes |
| Stage 2 Low-intermediate risk | Not stage 1 or 3 | |||
| Stage 3 High risk | More than 5.5 | High | High risk chromosomes | |
Symptoms of myeloma
The symptoms of myeloma depend on how advanced the disease is. In the earliest stages, there may be no symptoms, and myeloma is picked up during a routine blood test. However, in the more advanced stages of disease, there are likely to be some symptoms.
Common symptoms of myeloma
- Bone pain – usually in the back, ribs, hips or skull.
- Easily broken bones – usually without a cause, often involving the ribs or spine.
- Frequent infections or fevers – usually without an obvious cause. This occurs due to the abnormal immunoglobulins.
- Tiredness, rapid heart rate, shortness of breath, pale skin – symptoms of a low red blood cell (RBC) count, anaemia.
- Bruising and bleeding easily – due to a low platelet count.
- Feeling sick, drowsy, or confused – caused by elevated blood calcium.
- Changes to your urination habits – due to kidney damage caused by the myeloma.
Diagnosis of myeloma
Tests used to diagnose myeloma
- Medical history and physical exam.
- Blood tests – full blood count (FBC), kidney and liver function, electrolytes, serum free light chain, cytogenetics, beta-2 microglobulin, albumin, lactate dehydrogenase (LDH).
- Urine tests.
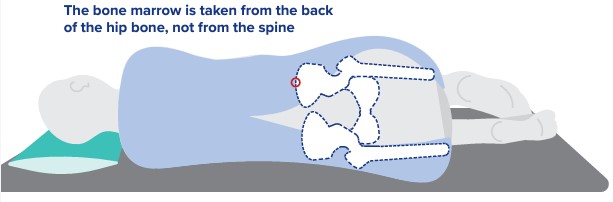
- Bone marrow biopsy.
- Imaging tests – may include a skeletal survey, computed tomography (CT) scan, positron emission tomography (PET) scan, magnetic resonance imaging (MRI).
Types of myeloma
Types of myeloma are classified based on the type of paraprotein produced by the myeloma cells.
Click on the headings below to learn more about the different types of myeloma.
Typical myeloma is the most common type of myeloma and is often referred to as just myeloma. This type of myeloma can be classified by the paraprotein it produces. They are made up of one type of heavy chain and one type of light chain.
There are five types of heavy chain immunoglobulins (Ig):
- IgG
- IgA
- IgD
- IgE
- IgM.
There are two types of light chain immunoglobulins:
- kappa
- lamba.
In typical myeloma, the heavy chain is bound to the light chain to form the paraprotein. It is most often present in the blood but not the urine. Blood tests are a good way to monitor this type of myeloma. When the myeloma is active, there will be a rise in the paraprotein level. When the myeloma is responding to treatment, there will be a decrease in the paraprotein level. However, it is normal for the paraprotein to fluctuate a little bit. A small rise does not always mean that more or different treatment is needed.
Light chain myeloma occurs in about 15% of people with myeloma. It is also known as Bence Jones myeloma. In light chain myeloma, myeloma cells only produce the light chain part of immunoglobulin. Not the heavy chain part. This is mostly detected in the urine. Small increases in the number of light chains in the blood can be detected through a blood test. This is called a serum free light chain test. This test can be used to see how you are responding to treatment. It is also used to look at the kappa and lamba light chain ratio. Everyone will have some free light chains in their blood. When these rise above normal levels, monitoring is required.
Non-secretory myeloma occurs in about 3% of people with myeloma. This type of myeloma produces no measurable paraprotein, so it cannot be detected in blood or urine tests, making it difficult to diagnose and monitor. Therefore, bone marrow biopsies and PET scans are used to diagnose and monitor this type of myeloma.
Precancerous conditions that can lead to myeloma
Some people develop early, precancerous conditions that can increase the risk of myeloma. However, most people with these conditions never develop myeloma and regular monitoring helps doctors detect changes early.
Click on the headings below to learn more about precancerous conditions that can lead to myeloma.
- MGUS is a disorder of the plasma cells.
- People with MGUS produce an abnormal protein called an M-protein rather than antibodies.
- The M-protein can build up in your blood stream and urine.
- The M-protein reduces your body’s ability to fight infection.
- MGUS doesn’t require any treatment, but monitoring is recommended.
- About 20% of people with MGUS develop myeloma.
- Is an early sign that you may develop myeloma after some time.
- Does not usually present many symptoms that affect you.
- Can be discovered through a blood test.
- Is managed by monitoring for signs and symptoms of active myeloma.
- Tends to affect people over 60.
- May develop into active myeloma during the five years after diagnosis for 10% of people with smouldering myeloma.
- Happens when plasma cells turn into abnormal cells, multiply and become a tumour that affect your bones.
- Appears only in one spot.
- It is often treated with radiotherapy.
- Can develop into myeloma for approximately 50% of people with solitary plasmacytoma.
- Happens when plasma cells turn into abnormal cells, multiply and become a tumour that affects the soft tissue.
- Tends to affect the tissue of your upper respiratory tract.
- Can be treated with surgery, chemotherapy, or immunotherapy.
- Could develop into myeloma for approximately 15% of people.
Treatment of myeloma
Your haematologist will recommend treatment based on:
- your diagnosis
- your age
- other health conditions
- physical condition
- your wishes.
Active treatment usually involves a combination of medications. This is because each medication acts on myeloma cells in a different way. The SLiM-CRAB criteria are used to work out if you have active myeloma that needs treatment, for instance.
SLiM-CRAB:
- S – sixty percent (60%) or more abnormal plasma cells in the bone marrow
- Li – light chains, high levels in the blood
- M – MRI with more than one bone abnormality
- C – calcium, high levels in the blood
- R – renal (kidney) damage
- A – anaemia, low red blood cell count
- B – bone lesions or fractures.
The aim of treatment is to:
- reduce the amount of myeloma in the body
- control any symptoms you are experiencing
- keep the myeloma under control for as long as possible
- improve your quality of life
- prolong your life.
Click on the treatments below to learn more.
Active monitoring (watch and wait) involves regular blood tests and general health checks. No intervention is needed unless you develop signs and symptoms to suggest the myeloma is progressing. People with smouldering myeloma and MGUS are generally actively monitored.
Most myeloma treatment regimens use steroids. They can be used on their own. Most commonly they are given with chemotherapy, targeted therapy or immunotherapy.
Steroids can:
- actively kill myeloma cells
- help other myeloma treatments be more effective
- act as an anti-inflammatory for people with myeloma bone disease
- act as an anti-nausea medication
- manage allergic type reactions to other myeloma medications.
During active treatment you will likely receive many courses of steroids. Dexamethasone and prednisolone are two types of steroids used in myeloma treatments. Dexamethasone is a strong steroid that is very good at killing myeloma cells. On the other hand, it has some side effects that can be hard to manage. While prednisolone also kills cancer cells, generally the side effects are better tolerated.
The main side effects of dexamethasone and prednisolone are:
- stomach pain
- high blood sugar levels
- mood changes
- difficulty sleeping
- fluid retention
- energy changes
- increased appetite and weight gain.
Speak with your treatment team if you are experiencing any of these side effects.
Targeted therapy is designed to attack specific genetic abnormalities in cancer cells to stop the cancer cell from growing. Unlike chemo, targeted therapy only affects the cells that have the abnormality. You may be prescribed a targeted therapy called a proteasome inhibitor. These are often given in combination with other medications.
Proteasome inhibitor examples
- bortezomib
- ixazomib
- carfilzomib.
These work by:
- breaking down excess proteins in cells to stop growth and development
- blocking the proteasomes so that proteins build up in the cell and the cell dies
- being given either subcutaneously (under the skin), intravenously (IV) or orally.
Side effects from targeted therapies tend to be different to chemo side effects. If you’re having more than one type of drug, you may have a few different side effects at different times. Your treatment team will talk to you about what you might expect.
You can read more about targeted therapy and specific side effects on this webpage Immunotherapies and targeted therapies | Leukaemia Foundation
Immunotherapy uses the immune system to recognise cancer cells and destroy them. Monoclonal antibodies and immune system modulators, for example, are two types of immunotherapies given in myeloma. These can be given in combination with other medications.
Monoclonal antibodies
- Daratumumab and Elotuzumab are examples of monoclonal antibodies given for myeloma.
- Daratumumab acts on monoclonal anti-CD38 antibody.
- Daratumumab targets the CD38 protein on myeloma cells, so the immune system recognises it and kills the cell.
- Elotuzumab acts on a myeloma cell protein called SLAMF7.
- Elotuzumab stimulates your immune system to recognise and kill myeloma cells.
Immune system modulators
- Thalidomide, lenalidomide, and pomalidomide are examples of immune system modulators given for myeloma.
- They stimulate the immune system to attack and destroy cancer cells.
- They directly kill and stop the growth of cancer cells.
- They can block the growth of new blood vessels that supply cancer cells.
Side effects from immunotherapies tend to be different to chemo side effects. If you’re having more than one type of drug, you may have a few different side effects at different times. Your treatment team will talk to you about what you might expect.
You can read more about immunotherapy and specific side effects on this webpage Immunotherapies and targeted therapies | Leukaemia Foundation
Chemotherapy (chemo) treatment for myeloma is often combined with other medications such as corticosteroids, immunotherapies or proteasome inhibitors.
Common chemotherapies used to treat myeloma include:
- melphalan
- doxorubicin
- cisplatin
- cyclophosphamide.
Chemo is given through a drip into the vein (intravenous) or by taking a tablet. It is therefore possible to have lots of side effects when you are having chemo. Each chemo has different risks. Ask your treatment team about the specific risks of the chemo they have prescribed for you.
Some more well-known side effects of chemo are:
- nausea and vomiting
- constipation and diarrhoea
- losing interest in food and eating
- chemo brain
- tiredness that you can’t shake
- infection.
Read about how to manage some of these side effects. Tell your treatment team if you are not feeling well or are not coping.
Myeloma can be treated with an autologous stem cell transplant. It is a treatment that restores stem cells after high dose chemotherapy. An autologous stem cell transplant means that you receive your own stem cells. There are times when myeloma is treated with an allogeneic stem cell transplant. The stem cells you receive in an allogeneic transplant are from a donor. Your treatment team will let you know if this is an option for you.
For more information visit: Stem cell transplants – Leukaemia Foundation
Radiation therapy is a local treatment that uses high energy rays to kill or damage cancer cells. It can be used to treat myeloma and plasmacytomas that are causing problems like pain and bone fractures.
Radiation therapy is used in myeloma to:
- relieve and reduce bone pain
- shrink the amount of myeloma cells in the bones to slow down bone damage
- target specific growths, lumps or areas that need treatment without affecting the whole body.
- treat in combination with other treatment
- prevent complications like further bone damage.
For more information visit: Radiation therapy – Leukaemia Foundation
Supportive care controls symptoms of myeloma and side effects of treatment. It aims to improve your quality of life but does not intend to treat the disease. It can help with symptoms such as tiredness, breathlessness, bruising or bleeding and high blood calcium.
Supportive care may include:
- blood transfusions
- platelet transfusions
- bisphosphonates.
For more information go to: Supportive care – Leukaemia Foundation
Bisphosphonates
Bisphosphonates are drugs that are used to strengthen and protect the bones. People with myeloma are at a high risk for developing bone fractures. This is because the balance between building new bone and bone loss is uneven. As a result, people with myeloma experience more bone loss than bone growth.
This leads to;
- osteoporosis
- lytic lesions (holes in bones)
- bone pain
- high levels of blood calcium
- bone fractures.
Regular treatment with bisphosphonates can reduce the risk of:
- bone pain
- high levels of blood calcium
- bone fractures.
Bisphosphonate therapies include:
- zoledronic acid – 15 minute infusion through a vein
- pamidronate – 90 minute infusion through a vein
- clodronate – tablets taken twice a day.
Bisphosphonates have some side effects including:
- flu like symptoms
- muscle and joint aches and pains
- low blood calcium, phosphate and magnesium levels
- osteonecrosis of the jaw (ONJ).
- read more about ONJ on our supportive care webpage.
You need to have a dental assessment and any dental treatment before starting bisphosphonates. Regular dental reviews and blood tests might also be required during treatment. Tell your treatment team if you experience any side effects.
Monitoring myeloma
Your treatment team will monitor your myeloma depending on your type of myeloma and the aim of treatment. Blood tests are taken frequently to see how you are responding to treatment. Your haematologist may be looking for the number of light chains in the blood or the kappa lamba light chain ratio. You may also have bone marrow biopsies, bone scans, PET scans and CT scans. After a period of remission however, your myeloma may relapse. This news can be difficult to hear and your treatment team will discuss your options with you. It’s important to seek support from those closest to you.
To speak to a Leukaemia Foundation Healthcare Professional call 1800 620 420 or get in touch via email at [email protected].
Living with myeloma
Myeloma treatments can be good at slowing down the disease, controlling symptoms and improving your quality of life for instance. Living with myeloma is different for everyone so it’s important to seek support from your loved ones so they can help you along your treatment journey.
Caring for someone with myeloma
We have a range of information and resources that may help when you are caring for someone with myeloma.
Resources for myeloma
Booklet to download:
Optimal Care Pathway for myeloma
An Optimal Care Pathway for myeloma has been developed in association with the Cancer Council, Australia and you can access it below.
Your Guide to Best Cancer Care – for multiple myeloma patients
A guide to help you, your family, and friends as you navigate through the healthcare system
References
- American Journal of Hematology | Blood Research Journal | Wiley Online Library
- Impact of HIV on Clinical Presentation and Outcomes of Individuals with Multiple Myeloma | Blood | American Society of Hematology
- IMWG Criteria for the Diagnosis of MM | Inl Myeloma Fn
- Monoclonal Gammopathy of Undetermined Significance – StatPearls – NCBI Bookshelf
- MSAG_Myeloma-Clinical-Practice-Guideline-2022_Final-1.pdf
- Multiple myeloma: EHA-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up† – Annals of Oncology
- Multiple Myeloma: 2022 update on Diagnosis, Risk-stratification and Management – PMC
- SLiM-CRAB Criteria I Multiple Myeloma Clinical Trials
- Second Revision of the International Staging System (R2-ISS) for Overall Survival in Multiple Myeloma: A European Myeloma Network (EMN) Report Within the HARMONY Project | Journal of Clinical Oncology
