About mantle cell lymphoma (MCL)
In MCL, the abnormal B lymphocytes:
- Become larger than they should and look different to healthy B-lymphocytes
- Won’t work effectively to fight infection
- Can spread to other parts of the body such as the blood, bone marrow and digestive track
MCL is usually an aggressive lymphoma. However, some people are diagnosed with an indolent MCL. MCL is currently not curable, but treatments are effective at keeping the lymphoma under control.
Who gets MCL
- MCL accounts for about 5-10% of all NHLs
- In 2020, there were 330 cases of MCL diagnosed in Australia
- It is more common in men than in women
- It mostly affects people over 60
Causes of MCL
MCL is mainly caused by genetic mutations that happen over your lifetime. These mutations change how your B-lymphocytes function. There is no exact cause for these genetic changes. There are some things that increase your risk of developing MCL. These include:
- Age – people over the age of 60 are more at risk
- Ethnicity – people of European background are more at risk
Symptoms of MCL
MCL may not cause any symptoms in the early stages. But as the lymphoma progresses, symptoms are likely to include:
- Painless swelling in the neck, armpit or groin
- Fevers without infection
- Tired for no reason
- Weight loss without trying
- Pain or full feeling in the abdomen
Diagnosis of MCL
MCL is diagnosed with a number of tests. You may have some or all these tests before an accurate diagnosis can be made.
Medical history and physical exam
Your haematologist will check:
- How you’ve been feeling
- Your symptoms and how long you’ve been experiencing them
- Your health history and your family’s health history
.
You will have a physical exam to check for any swelling or pain around your neck, armpits and groin. Tell your haematologist if you’ve noticed any changes in your body.
Blood tests
Blood tests are taken:
- At diagnosis (baseline bloods) and throughout treatment.
- To see if MCL is affecting your blood cells, electrolytes, or other organs such as the liver or kidneys.
Once you start treatment, blood test results are compared with your baseline results to see how you are responding to treatment.
Lymph node biopsy
A biopsy is a surgical procedure to remove some tissue from the body for testing. In MCL, a lymph node biopsy involves removing part or all of a suspicious lymph node. Depending on the area and how much tissue is taken for the biopsy you may be given local anaesthetic, or it may be performed under a general anaesthetic. The tissue is sent to the laboratory (pathology) for testing. The purpose of a lymph node biopsy is to confirm your diagnosis, identify your subtype of MCL, and develop a treatment plan.
Genetic tests
- Genetic tests look for faults in the cancer cells
- In MCL, a piece of chromosome 11 swaps places with a piece of chromosome 14. This is called translocation.
- This translocation turns on a gene that tells B-cells to grow uncontrollably.
- This translocation is found in more than 90% of people with MCL.
- Genetic tests are done on your collected blood and bone marrow samples
- The tests are called: FISH (fluorescence in situ hybridisation) and PCR (polymerase chain reaction).
Staging tests
Your haematologist may ask you to have some staging tests to see if MCL is in other parts of your body. Staging helps determine your prognosis and treatment. These tests might include:
- Computed tomography (CT) scan
- Positron emission tomography (PET) scan
- Ultrasound
- Bone marrow biopsy
These tests can also be used to see how you are responding to treatment. You can read more about these imaging tests in Non-Hodgkin lymphoma (NHL) – A guide for people with NHL
Types of MCL
The World Health Organization (WHO) has a system that defines MCL subtypes. Your haematologist will use the WHO system to work out your subtype and treatment. There are two main types of MCL:
- Classical MCL – Starts in your lymph nodes and usually spreads to other areas of the body. It is usually quite aggressive. Most cases of MCL are this type.
- Leukaemic non-nodal MCL – This type is slower growing. It can cause a swollen spleen, and you will usually have lymphoma cells in your blood and bone marrow.
Staging MCL
Staging describes how far the lymphoma has spread throughout the body. Your stage of MCL will depend on:
- How many areas of the body are affected by the lymphoma
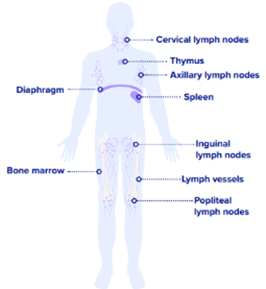
- If the lymphoma is above and/or below the diaphragm
- Whether the lymphoma has spread to the bone marrow or other organs.
| Stage 1 lymphoma Lymphoma is only in one lymph node area, or one organ such as the thymus, or one area of a single organ outside the lymphatic system. |
| Stage 2 lymphoma Lymphoma affects two or more lymph node areas either above or below the diaphragm* or extends locally from one lymph node area into a nearby organ. |
| Stage 3 – 4 lymphoma Lymphoma is in lymph node areas on both sides of the diaphragm*(stage 3), or the cancer has spread throughout the body beyond the lymph nodes (stage 4). |
*the diaphragm is a large muscle that separates your stomach and chest.
Prognosis of MCL
A prognosis is an estimate your haematologist will make of the likely course and outcome of your disease. MCL is not curable, but there are treatments that can keep the lymphoma under control.
Treatment of MCL
Treatment for MCL depends on a few factors. It usually consists of a combination of medicines including immunotherapy and chemotherapy. Factors that are considered when planning treatment include:
- Your exact subtype of MCL
- Your stage of MCL
- If the MCL is indolent or aggressive
- Your age
- Your overall health
- Your wishes
Some treatment options for MCL
Chemotherapy
Chemotherapy (chemo) for MCL is often given in combination with immunotherapy.
- Chemo can be given as tablets, injections, or infusions via a drip (IV)
- Chemo is given in cycles of treatment days. This means that you will have treatment for a certain number of days, followed by a set number of rest days
- Chemo cycle times depend on the drugs in your treatment. The number of treatment days and the number of cycles depend on the disease and drugs
- Examples of chemo treatment plans for MCL:
- R-CHOP – Rituximab, doxorubicin, vincristine, cyclophosphamide, prednisolone
- R-DHAP – Rituximab, dexamethasone, cytarabine, cisplatin
- R-maxi-CHOP – known as the Nordic protocol. The same treatments as R-CHOP but at higher doses
- Hyper-CVAD – complex chemo regimen consisting of part A and part B
- BR – Bendamustine and rituximab
The higher dose treatments, such as R-maxi-CHOP and Hyper-CVAD are given in hospital. They are complex treatments that require monitoring. Other treatments can be given in a day infusion center.
Chemo side effects can vary. Read more about the general side effects of chemotherapy.
Immunotherapy
Immunotherapy is a type of biological treatment that helps the immune system recognise and destroy cancer cells. It is often given in combination with chemotherapy.
In MCL:
- The cancerous B-cells have a protein called CD20 on their surface.
- CD20 is also found on normal B-cells.
- When this protein is present, it’s called CD20-positive lymphoma.
Monoclonal anti-CD20 antibody, Rituximab, targets the CD20 protein on B-cells. It works by attaching to the CD20 protein on the surface of the cancerous B-cell. This signals the immune system to destroy the cell, helping to control the cancer.
Targeted therapy
Targeted therapy is a type of cancer treatment:
- That targets cell markers or pathways that control how cancer cells grow, divide, and spread
- Specific to a genetic abnormality within the cancer cell. The drug targets that abnormality, also called a cell marker, to stop the cancer cell from growing
- Only affects the cells that have that cell marker
Bruton’s tyrosine kinase (BTK) is a protein that is important for the growth of B-cells. In MCL, BTK is disrupted due to genetic changes, leading to out-of-control growth of B-cells. Zanubrutinib is a BTK inhibitor (BTKi) that blocks the B-cell receptor on cancer cells, causing them to die. You might receive Zanubrutinib if your MCL has come back after a period of remission.
Side effects of targeted therapy and immunotherapy are different to chemo side effects. You can read more about them here: Immunotherapies and Targeted therapies.
Stem cell transplant
A bone marrow or blood stem cell transplant is a treatment that restores stem cells after high dose chemotherapy. Your treatment team might suggest a transplant if your MCL is aggressive, difficult to treat, has relapsed, transformed or is refractory. There are two types of transplants:
- An autologous stem cell transplant – your own stem cells are collected and then given back to you after high dose chemotherapy.
- An allogeneic stem cell transplant – you receive stem cells from a donor, often a blood relative.
Clinical trials
Clinical trials (also called research studies) test new treatments and often provide early access to promising therapies that aren’t routinely available. Results from the new agent (or combination of agents) are compared against current (or standard) treatments to see if the new treatment works better. They also check for side effects from the new treatment. Your haematologist may suggest you join a clinical trial.
Follow-up care
You will need regular checkups with your treatment team once you have commenced treatment for your MCL. This is to check on how the MCL is tracking and any long-lasting side effects from the treatment. If you notice any symptoms of your MCL returning after you commence treatment, you should tell your treatment team as soon as possible. You may need tests if you have symptoms to check the lymphoma isn’t progressing. It is possible you may require a change of treatment to keep the lymphoma under control.
Living with MCL
How MCL affects your everyday life will depend on many factors. It could be that you are returning or managing work, trying to exercise or managing your nutrition. There are some helpful resources and information to guide you – Living well with blood cancer.
Caring for someone with MCL
We have a range of information and resources that may help when you are caring for someone with mantle cell lymphoma (MCL).
Resources for MCL
Booklets to download:
The non-Hodgkin lymphoma booklet may provide information relevant to anyone diagnosed with mantle cell lymphoma (MCL).
-

Non-Hodgkin lymphoma (NHL) information booklet
pdf / 1.33 MB
The NHL booklet has been translated into the following languages:
-
Non-Hodgkin lymphoma (NHL) information booklet – Arabic [العربية]
pdf / 10.88 MB
-
Non-Hodgkin lymphoma (NHL) information booklet – Filipino [Pilipino]
pdf / 10.81 MB
-
Non-Hodgkin lymphoma (NHL) information booklet – Greek [Ελληνικά]
pdf / 10.89 MB
-
Non-Hodgkin lymphoma (NHL) information booklet – Hindi [हिंदी]
pdf / 11.09 MB
-
Non-Hodgkin lymphoma (NHL) information booklet – Simplified Chinese [简体中文]
pdf / 11.35 MB
-
Non-Hodgkin lymphoma (NHL) information booklet – Traditional Chinese [繁體字]
pdf / 11.77 MB
-
Non-Hodgkin lymphoma (NHL) information booklet – Vietnamese [Tiếng Việt]
pdf / 10.90 MB
Optimal Care Pathway for low grade lymphoma
An Optimal Care Pathway for low grade lymphoma has been developed in association with the Cancer Council, Australia and you can access it below.
Your Guide to Best Cancer Care – for low grade lymphoma patients
A guide to help you, your family, and friends as you navigate through the healthcare system
References
- Mantle Cell Lymphoma (MCL) – Lymphoma Australia
- Mantle Cell Lymphoma: Symptoms, Treatment & Prognosis
- Mantle Cell Lymphoma – StatPearls – NCBI Bookshelf
- What is mantle cell lymphoma? Magda Szubanski’s ‘rare and fast-moving’ cancer, explained
- Mantle Cell Lymphoma – Symptoms, Causes, Treatment | NORDMantle Cell Lymphoma Stages and Treatments
